Last updated on June 3, 2026
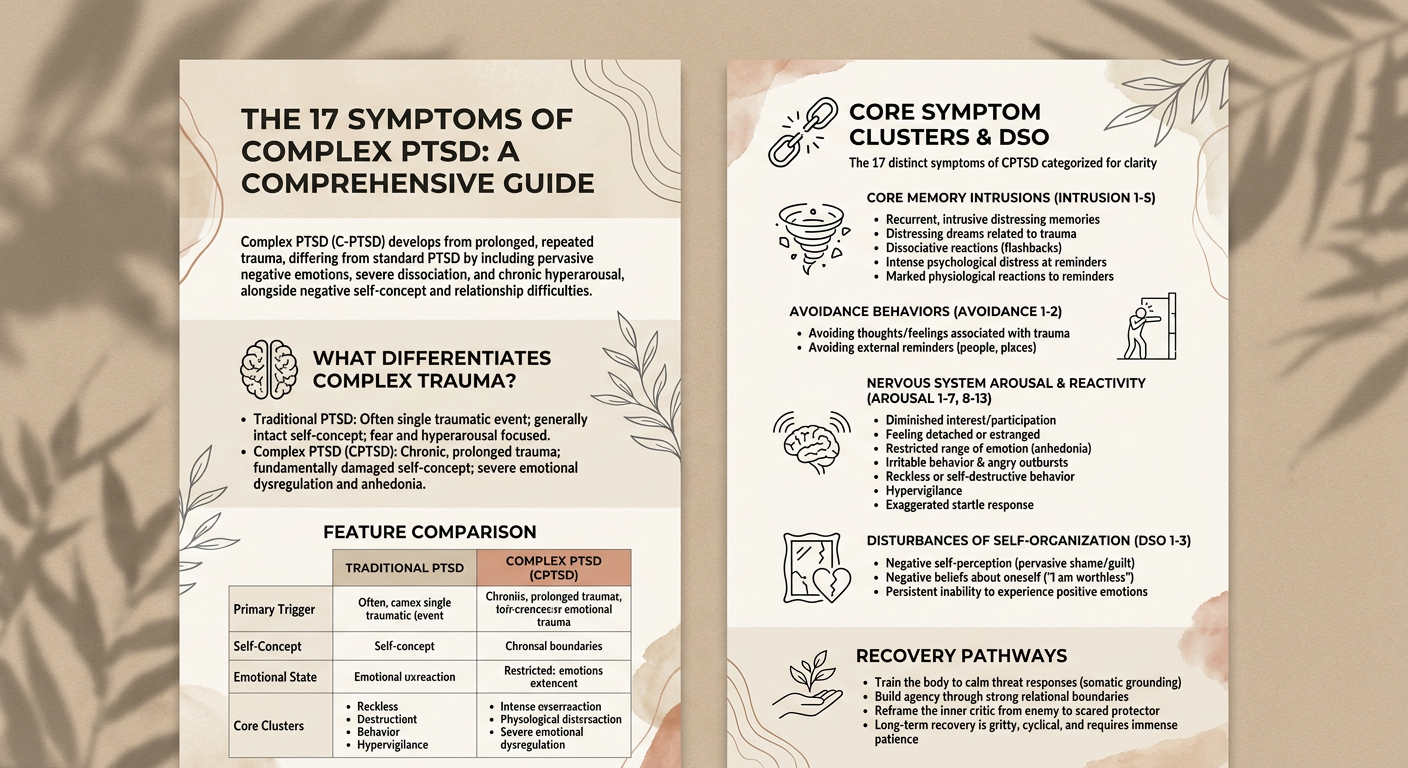
Complex PTSD (C-PTSD) is characterized by 17 distinct symptoms that develop from prolonged, repeated trauma, setting it apart from standard PTSD. These symptoms include pervasive negative emotions, severe dissociation, and chronic hyperarousal. Individuals may also experience negative changes in self-concept, persistent feelings of shame, and difficulties in maintaining relationships. This comprehensive guide outlines these 17 symptoms to provide a clear understanding of Complex PTSD and its necessary specialized approach to recovery.
Finding solid information online can be a frustrating process. You often scour endless pages, click through broken submenu links, and enter your zip code trying to find a local health professional or medical center. Half the time, you just land on an advertisement, or clinic sponsored page that barely scratches the surface of actual trauma recovery. That ends today. We are going to break down the reality of this disorder, stripping away the clinical jargon to uncover what these behavioral stress responses actually look like on the ground.
What Differentiates Complex Trauma From Traditional Diagnoses?
If you’ve spent any time looking for answers about complex post, you’ve probably hit a wall of clinical gatekeeping. People get incredibly stuck arguing about the diagnostic and statistical manual of mental disorders. The reality is that complex ptsd isn’t formally listed as a distinct diagnosis in the DSM-5. This causes a massive headache for clinicians and survivors alike, often resulting in an error outline of a patient’s true struggles.
I frankly obsess too much over what labels a system uses if the therapy actually helps. But I do care when the medical system hides behind diagnostic manuals to avoid learning about pervasive trauma patterns. Fortunately, the global medical community defines Complex PTSD separately from traditional PTSD. The world health organization explicitly outlines it in the international classification of diseases 11 th revision (icd 11). They look at a specific category called disturbances of self-organization, commonly referred to as DSO symptoms.
Traditional PTSD usually stems from a single traumatic event. Think of a severe vehicle accident or a sudden natural disaster. Complex trauma is a different animal. It’s chronic. It’s the slow, unrelenting burn of childhood trauma, long term trauma, severe neglect, or sexual abuse. It fundamentally shifts how you perceive yourself.
Clinicians frequently misdiagnose these extensive issues. Because the medical system struggles with the severity of complex traumas, you’ll see people incorrectly shuffled into categories for borderline personality disorder (bpd), dissociative ptsd, or even autism. But while borderline personality disorder heavily features a frantic fear of abandonment, cptsd is deeply rooted in avoiding catastrophic threats to the self.
| Feature | Traditional PTSD | Complex PTSD (CPTSD) |
|---|---|---|
| Primary Trigger | Single traumatic experience | Prolonged, chronic trauma |
| Self-Concept | Generally intact, though shaken | Fundamentally damaged, pervasive shame |
| Emotional State | Fear and hyperarousal focused | Severe emotional dysregulation, anhedonia |
| Core Clusters | Intrusion, Avoidance, Arousal | PTSD clusters + DSO symptoms |
To get a clear picture of the full scope of these disorders, please review this comprehensive, numbered list of all 17 symptoms of CPTSD:
- Intrusion (1-5): Recurrent, involuntary, and intrusive distressing memories
- Intrusion (2): Recurrent distressing dreams related to the trauma
- Intrusion (3): Dissociative reactions (flashbacks) where the individual feels as if the trauma were recurring
- Intrusion (4): Intense or prolonged psychological distress at internal or external reminders
- Intrusion (5): Marked physiological reactions to reminders (e.g., heart rate, sweating)
- Avoidance (1-2): Avoiding memories, thoughts, or feelings associated with trauma
- Avoidance (2): Avoiding external reminders (people, places, conversations, objects)
- Arousal & Reactivity (1-7): Markedly diminished interest or participation in significant activities
- Arousal & Reactivity (8): Feeling detached or estranged from others
- Arousal & Reactivity (9): Restricted range of emotion (inability to have loving feelings)
- Arousal & Reactivity (10): Irritable behavior and angry outbursts
- Arousal & Reactivity (11): Reckless or self-destructive behavior
- Arousal & Reactivity (12): Hypervigilance
- Arousal & Reactivity (13): Exaggerated startle response
- DSO (1): Negative self-perception (pervasive shame/guilt)
- DSO (2): Negative beliefs about oneself (e.g., “I am worthless”)
- DSO (3): Persistent inability to experience positive emotions
Core Memory Intrusions And Avoidance Behaviors
These are the baseline ptsd symptoms, the foundational stress responses that both traditional and complex diagnoses share.
Intrusive Flashbacks And Memories
You don’t just remember a traumatic experience. You physically relive it. The base symptoms of PTSD include intrusive thoughts that violently hijack your current reality. Your brain simply hasn’t filed the memory away in the past tense. A specific smell, a sudden tone of voice, or a passing shadow can rip you out of the present moment. Your nervous system plunges back into survival mode, reacting as if the abuse is happening right now.
Chronic Sleep Nightmares
Sleep is supposed to be restorative. For someone carrying a heavy trauma load, lying in the dark is when the psychological defenses finally drop and the brain starts running worst-case scenarios. Chronic sleep nightmares are relentless. You wake up sweating, your heart hammering against your ribs, entirely unsure of what year it is or where you are. This isn’t just a bad dream. It’s your brain desperately trying to process unresolved threat responses while you are unconscious.
Internal And External Avoidance
You learn to build walls quickly. Avoidance takes two forms. External avoidance is obvious. You dodge specific people, sidestep physical locations, or refuse to engage in activities that act as distressing reminders. Internal avoidance is much sneakier. You actively shut down your own thoughts. You numb out. If you don’t feel anything, you can’t be hurt by anything.
Nervous System Arousal And Dissociation States
When the body believes it is constantly under attack, it adapts. These symptoms showcase how traumatic stress rewires the physical architecture of the brain.
Constant Threat Hypervigilance
Imagine a fire alarm that never turns off. That is your brain on chronic trauma. Your body is stuck in a state of constant threat hypervigilance. Studies analyzing the biological effects of childhood trauma show how chronic stress fundamentally alters your neurochemistry over time. You are utterly exhausted yet fiercely on guard. You scan every room for exits. You analyze every subtle shift in a friend’s facial expression, waiting for the inevitable betrayal.
Exaggerated Startle Responses
Someone drops a fork in a quiet restaurant, and you nearly jump up. Exaggerated startle responses betray a nervous system that has lost its inhibitory control. Scientific breakdowns exploring the molecular and cellular effects of traumatic stress reveal how communication loops in the prefrontal cortex get disrupted. Your brain literally loses the ability to safely extinguish fear memories. You live in a constant state of physiological flinching.
Depersonalization And Somatic Pain
Sometimes the brain’s only escape route is to detach entirely. Dissociation often manifests as depersonalization. You feel completely disconnected from your own body, watching yourself move from a million miles away. This isn’t purely psychological. Trauma takes a massive toll on the autonomic nervous system. Hard data looking at neuroimaging and brain volume shifts shows actual structural alterations in the brain. That translates into real somatic pain. Chronic headaches, severe stomach aches, and inexplicable muscle tension are deeply intertwined with this mental health condition.
Emotional Dysregulation And Self-Concept Deficits
This is where we cross into the unique territory of the 11 th revision diagnostic criteria. The disturbances in affect regulation define the CPTSD experience.
Pervasive Emotional Anhedonia
You stop caring about the things that used to light you up. Pervasive emotional anhedonia is an incredibly isolating symptom. It’s not just feeling a little sad. It’s a profound, hollow emptiness. You go through the motions of a hobby, a job, or a relationship, but the internal reward system is offline. The world feels entirely muted.
Reactive Anger And Despair
When the numbness finally breaks, it usually shatters into overwhelming intensity. Emotional dysregulation goes completely out the window. Papers by researchers like carmassi c emotional dysregulation patterns consistently highlight this instability. One moment you are perfectly fine. The next, a minor inconvenience sparks blind, reactive anger or bottomless despair. It’s entirely unpredictable.
Pervasive Toxic Shame
This is the heavy anchor pulling everything down. Pervasive toxic shame isn’t feeling bad about a specific mistake. It’s the deeply held conviction that you are a mistake. It is a fundamental defectiveness. You carry this unshakable belief that you are irreparably broken, forever contaminated by your past.
Interpersonal Isolation And Worthlessness Indicators
Trauma sustained in relationships inevitably damages your ability to connect with others. The interpersonal fallout is often the most painful part of the disorder.
Persistent Chronic Guilt
You take the blame for everything, even situations entirely outside your control. Persistent chronic guilt is a survival mechanism gone rogue. If a child experiences severe abuse, their brain often decides it’s safer to believe they caused the trauma rather than accept that their caregivers are dangerous monsters. You carry that misplaced responsibility directly into adulthood.
Severe Feelings Of Worthlessness
When toxic shame and chronic guilt merge, they breed severe feelings of worthlessness. You genuinely believe you do not deserve good things, healthy relationships, or even basic kindness. It feels safer to reject yourself before anyone else gets the chance to do it for you.
Deep Interpersonal Boundary Impairments
Surviving often meant keeping dangerous people happy. That translates into deep interpersonal boundary impairments. You fawn. You people-please. You tolerate abusive dynamics because your nervous system learned long ago that saying “no” results in punishment.
Train The Body To Calm Threat Responses
A lot of people walk into therapy thinking they just need to think differently. They try to logic their way out of a panic attack. Let me be blunt. If you don’t train the body, you are basically arguing with a fire alarm. You can have all the intellectual insight in the world and still freeze, fawn, or rage because your nervous system is running the show.
Recovery starts with building tolerance for physical sensations that would normally terrify you. A faster heartbeat during a workout doesn’t automatically mean you are in imminent danger. You have to intentionally practice grounding and soothing techniques.
- Notice the physical trigger without immediately reacting.
- Implement a somatic grounding technique, like deep breathing or temperature shifts.
- Acknowledge the physical discomfort without attaching a catastrophic narrative to it.
- Proceed with the safe activity, proving to your body that the threat is false.
Your brain needs to learn that being uncomfortable isn’t the same as being unsafe. Clinical guidelines dictating evidence-based treatments like Cognitive Processing Therapy consistently emphasize regulating the physical stress response before you even attempt to tackle the cognitive distortions. Modalities like emdr can also help process these frozen somatic states.
Build Agency Through Strong Relational Boundaries
People in long recovery communities usually circle back to one core concept: agency. It’s the ability to spot red flags and actually walk away without feeling like you are abandoning yourself. If someone tells you they “can’t set boundaries,” it usually means their system learned that self-advocacy is a punishable offense.
Setting a boundary isn’t a personality upgrade. It’s survival math. Recovery looks like shrinking the gap between noticing you’re uncomfortable and taking action to protect yourself, even while your hands are shaking. You practice doing the scary thing in small, tolerable doses until your system stops treating it like a life-or-death confrontation. Use the official trauma treatment guidance from NICE as a framework to understand what healthy, safe support should look like, whether in personal relationships or a clinical nhs setting.
How Does A Survivor Reframe The Inner Critic?
The voices in your head can be incredibly vicious. But the inner critic isn’t just cruelty. It is often a terrified manager trying to prevent danger through intense control and self-punishment. The helpful shift is realizing the critic’s job is protection, even if the method is brutally abusive.
The critic isn’t your enemy, but it certainly isn’t your therapist either. You have to learn to separate the “warning” from the “disgust.” A warning sounds like, “Hey, pay attention to this situation, it feels off.” Disgust sounds like, “You’re disgusting, stop existing.” Getting better means refusing to obey the disgust while still acknowledging the legitimate safety signals. Data from studies like liang y complex posttraumatic stress disorder prevalence suggest that managing this internal hostility is critical for long-term stabilization.
Conclusion
When I picture long-term recovery from complex post-traumatic stress disorder, I don’t picture one heroic, cinematic breakthrough. I picture repeated, gritty cycles. You notice a trigger a little earlier. You calm down a fraction sooner. You stop bargaining with the wrong relationships. You become less surprised that you’re simply human when you feel bad.
It is painfully slow at times because you are rewiring neural pathways built for survival, not comfort. The treatments require immense patience. You aren’t aiming to become “normal.” You are aiming to reclaim your own life, with fewer emergencies and a hell of a lot more choice. Stay stubborn. The work is absolutely worth it.